Being told your cornea is too thin for LASIK can feel like a door slamming shut — especially when you’ve been looking forward to life without glasses. But here’s what most patients don’t hear in that moment: a thin cornea only disqualifies you from one specific procedure. It doesn’t disqualify you from clear vision. Several modern alternatives bypass the cornea entirely or work with significantly less tissue, and some may actually be a better fit for your eyes than LASIK would have been.
This guide explains why corneal thickness matters for LASIK, what the actual minimum numbers are, and — most importantly — walks you through every alternative procedure available so you can make an informed choice rather than simply accepting “you’re not a candidate” as the final word.
Key Takeaways
- LASIK typically requires a minimum corneal thickness of 480–500 microns, with at least 250 microns of residual stromal bed after surgery.
- A thin cornea doesn’t mean you can’t have vision correction — it means you need a different procedure.
- SMILE Pro, ICL, TransPRK, and Refractive Lens Exchange are all proven alternatives for patients with insufficient corneal thickness.
- Advanced diagnostics (pachymetry, tomography) determine not just thickness but the overall structural safety of your cornea.
Why Does Corneal Thickness Matter for LASIK?
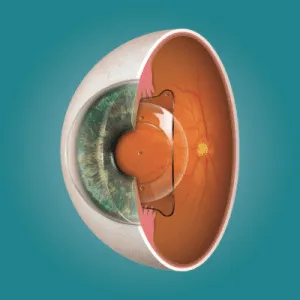
LASIK corrects vision by removing microscopic layers of corneal tissue with an excimer laser. Before the laser can do its work, a thin flap — typically 90 to 110 microns thick — is created in the cornea’s surface and folded back. The laser then reshapes the exposed stromal bed, and the flap is repositioned. Every dioptre of correction requires removing roughly 12 to 16 microns of tissue from this bed.
The problem with thin corneas is arithmetic. After the flap is created and the tissue is ablated, a minimum amount of untouched corneal stroma — called the residual stromal bed (RSB) — must remain to keep the cornea structurally stable. If too little tissue is left behind, the cornea can progressively weaken and bulge forward over months or years, a condition known as post-LASIK ectasia. Ectasia is one of the most serious complications in refractive surgery, and it’s almost entirely preventable through proper patient selection — which is exactly why corneal thickness screening exists.
It’s worth noting that thickness alone doesn’t tell the whole story. The shape, curvature, and internal structure of the cornea matter just as much. A cornea measuring 510 microns might be safe for one patient but risky for another if corneal topography reveals suspicious curvature patterns. This is why advanced imaging — not just a single pachymetry reading — is essential before any decision is made.
What Is the Minimum Corneal Thickness for LASIK?
Most refractive surgeons consider 480 to 500 microns the lower threshold for standard LASIK eligibility, though the more important number is the residual stromal bed after surgery, which should be at least 250 microns (many surgeons prefer 280–300 for an added safety margin). The average Indian cornea measures around 530 microns, so there’s typically enough tissue for moderate corrections. But for patients with corneas in the 460–490 range — or those who need high corrections that would remove a large amount of tissue — standard LASIK may not leave enough structural reserve.
A patient with a 520-micron cornea and −2.00 D of myopia has plenty of room. The same patient with −8.00 D may not, because the laser needs to remove significantly more tissue. This is why the maximum power LASIK can correct is directly tied to how much cornea you have to work with. Thickness and prescription together determine eligibility — neither number means much in isolation.
Safe Alternatives When Your Cornea Is Too Thin
SMILE Pro — Less Tissue, No Flap
SMILE Pro extracts a tiny disc of tissue (a lenticule) through a 2–4 mm keyhole incision — no flap is created. Because there’s no flap, less corneal tissue is consumed by the access step, meaning more stroma is preserved for structural integrity. For patients whose corneas fall just below the LASIK threshold — say 480 to 500 microns — SMILE Pro often provides enough margin to proceed safely. It treats myopia up to −10.00 D and astigmatism up to 5.00 D. For a detailed comparison of corneal tissue preservation, see our article on SMILE for thin corneas.
TransPRK — Surface Treatment, Zero Flap
TransPRK is a surface ablation procedure that treats the cornea without creating any flap or incision at all. The laser works directly on the corneal surface after removing the epithelium (which regenerates naturally within days). Because no tissue is “spent” on flap creation, TransPRK preserves the maximum possible stromal thickness — making it a strong option for patients with borderline corneas. The trade-off is a longer recovery: expect three to five days of discomfort and one to two weeks before vision fully sharpens. But for patients who value corneal safety above recovery speed, it’s an excellent choice.
ICL — Implantable Collamer Lens (No Corneal Tissue Removed)
When your cornea is definitively too thin for any laser procedure, ICL surgery changes the equation entirely. Instead of reshaping the cornea, a biocompatible lens is placed inside the eye — between the iris and the natural lens — to correct the refractive error. No corneal tissue is removed whatsoever, which means corneal thickness is no longer a limiting factor. ICL corrects myopia up to −18.00 D, hyperopia up to +10.00 D, and astigmatism up to 6.00 D. It’s also reversible: the lens can be removed or replaced if your needs change. For patients with both thin corneas and high prescriptions, ICL is often the safest and most effective path to glasses-free vision.
Refractive Lens Exchange (RLE)
For patients over 40 — especially those with thin corneas combined with early presbyopia or high hyperopia — refractive lens exchange may be the most practical solution. RLE replaces the eye’s natural lens with an artificial intraocular lens (IOL) that corrects the refractive error, much like cataract surgery but performed before a cataract develops. Because the procedure works inside the eye rather than on the cornea, corneal thickness is irrelevant. It also eliminates the possibility of needing cataract surgery later in life, since the natural lens has already been replaced.
Can Cross-Linking Help Thin Corneas?
Corneal cross-linking (C3R) strengthens the collagen bonds within the cornea, and some surgeons use it in combination with surface ablation (a protocol sometimes called “LASIK Xtra” or “CXL-plus”) to add structural reinforcement after laser correction on borderline corneas. This combined approach is still evolving and isn’t appropriate for everyone, but it has expanded the eligibility window for certain patients who would otherwise have been excluded from laser treatment entirely.
How to Choose the Right Alternative
The right procedure depends on more than just corneal thickness. Your age, prescription, lifestyle, and long-term visual goals all factor in. A 25-year-old with −5.00 D myopia and a 475-micron cornea might be ideal for SMILE Pro or TransPRK. A 30-year-old with −12.00 D and the same corneal thickness needs ICL — no laser procedure can safely correct that much power regardless of the approach. A 50-year-old with thin corneas and +4.00 hyperopia might be best served by refractive lens exchange.
At Visual Aids Centre, every patient undergoes a comprehensive diagnostic workup — including Pentacam tomography, pachymetry mapping, aberrometry, and dry eye assessment — before any procedure is recommended. The goal is never to fit you into a procedure. It’s to match the safest, most effective option to your specific anatomy and needs. If you’ve been told your cornea is too thin for LASIK, that evaluation is the essential next step — because the answer is almost never “nothing can be done.”
Conclusion
A thin cornea closes the door on standard LASIK — but it opens several others. SMILE Pro preserves more tissue by eliminating the flap, TransPRK works entirely on the surface for maximum stromal conservation, ICL bypasses the cornea altogether for high prescriptions, and refractive lens exchange solves the problem from inside the eye. The key is a thorough diagnostic evaluation that looks beyond a single thickness number and considers your full ocular anatomy. If you’ve been told your cornea is too thin, book a comprehensive assessment and find out which alternative gives you the clearest, safest path to life without glasses.
Frequently Asked Questions (FAQs)
What corneal thickness is too thin for LASIK?
Generally, corneas below 480 microns are considered too thin for standard LASIK. However, eligibility also depends on your prescription and the residual stromal bed calculation — not thickness alone.
Can I still get laser eye surgery with a thin cornea?
Yes. Surface procedures like TransPRK don’t require a flap and preserve more tissue. SMILE Pro also conserves more stroma than LASIK. Both can be viable for borderline corneas.
Is ICL safer than LASIK for thin corneas?
ICL doesn’t touch the cornea at all, making it the safest option when corneal thickness is a concern. It’s particularly well-suited for high prescriptions combined with thin corneas.
Can thin corneas get thicker over time?
Corneal thickness is largely stable in adults and doesn’t increase naturally. Some conditions like oedema can temporarily swell the cornea, but this doesn’t represent usable tissue for surgery.
What is the residual stromal bed (RSB) and why does it matter?
The RSB is the amount of corneal stroma left untouched after flap creation and laser ablation. A minimum of 250 microns is required to prevent ectasia — the progressive weakening and bulging of the cornea.
Is 460 microns too thin for any vision correction procedure?
Not at all. While 460 microns rules out standard LASIK, procedures like ICL, TransPRK, and in some cases SMILE Pro remain safe options. A full evaluation will determine which is right for you.
👁️ MEDICALLY REVIEWED BY
Padmashree Dr. Vipin Buckshey
Optometrist & Refractive Surgery Specialist | AIIMS Graduate, 1977 | Padma Shri Honouree
With more than four decades of clinical experience and over 250,000 laser vision correction procedures performed at Visual Aids Centre, Dr. Vipin Buckshey has evaluated thousands of patients with thin or borderline corneas — guiding each one toward the safest correction pathway based on comprehensive diagnostics, not a single measurement. An AIIMS alumnus, former President of the Indian Optometric Association, and official optometrist to the President of India, Dr. Buckshey ensures that no patient leaves the centre without understanding every option available to them. Learn more about our story and the clinical team behind Visual Aids Centre.