If you or your child has been diagnosed with a squint (strabismus), surgery isn’t always the first — or only — answer. Depending on the type, severity, and underlying cause of the misalignment, several non-surgical treatments can effectively correct or significantly improve a squint, especially when started early.
This guide walks you through every proven non-surgical option for squint eye treatment, explains who they work best for, and clarifies when surgery does become necessary. Whether you’re a parent researching options for a child or an adult dealing with intermittent misalignment, the information below will help you understand what’s available before you commit to the operating table. For a broader overview of the condition itself, our squint eye service page covers the clinical fundamentals.
Key Takeaways
- Non-surgical squint treatments include corrective glasses, prism lenses, vision therapy, patching, and Botox injections.
- Accommodative squints caused by farsightedness often resolve entirely with the right spectacle prescription.
- Vision therapy (orthoptics) is most effective for convergence insufficiency and intermittent squints in children and adults.
- Surgery becomes necessary when the deviation is large, constant, and unresponsive to conservative treatment.
What Is a Squint Eye (Strabismus)?
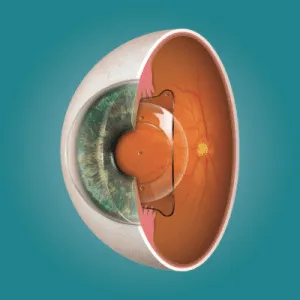
A squint — medically called strabismus — occurs when the six muscles controlling each eye’s movement don’t work in coordination. Instead of both eyes pointing at the same object simultaneously, one eye deviates inward, outward, upward, or downward while the other focuses normally. The brain receives two conflicting images, which can cause double vision in adults or, in children, lead the brain to suppress the weaker eye’s input entirely — a condition known as amblyopia (lazy eye).
Around 4–6% of India’s population has some form of strabismus, according to data from the National Institute of Ophthalmology. The condition is not merely cosmetic — left untreated, it can permanently impair binocular vision, depth perception, and the weaker eye’s visual acuity. The good news is that many cases respond well to non-surgical intervention, particularly when caught early.
Types of Squint and Why It Matters for Treatment
The direction and consistency of the deviation determine which treatments are viable. Understanding your specific type is the first step toward choosing the right approach.
Convergent Squint (Esotropia)
The eye turns inward. This is the most common type in children and is frequently linked to uncorrected farsightedness (hyperopia). Accommodative esotropia — where the eye turns in because it’s overworking to focus — often responds completely to corrective glasses without any further intervention.
Divergent Squint (Exotropia)
The eye drifts outward, typically becoming more noticeable when the person is tired, daydreaming, or looking at distant objects. Intermittent exotropia is particularly responsive to vision therapy and convergence exercises. To understand whether laser correction of an underlying refractive error could help, see our article on whether LASIK can reduce squint.
Vertical Squint
The eye turns upward or downward. Less common, and more likely to require surgical correction, though prism glasses can manage mild cases effectively.
Intermittent vs Constant
Intermittent squints — those that appear only under certain conditions like fatigue or illness — generally respond better to non-surgical treatment than constant, large-angle deviations. If the squint is present all the time, conservative approaches may still be tried first, but surgery is more likely to be needed. For context on surgical outcomes, our article on squint surgery success rates provides the data.
Common Causes of Squint in Children and Adults
In Children
The most frequent cause is an imbalance in the extraocular muscles, often present from birth (congenital strabismus) or developing in early childhood. Uncorrected refractive errors — particularly hyperopia — are a major contributor to accommodative squints. Genetics play a significant role: if a parent or sibling has strabismus, the risk increases substantially. Conditions like Down syndrome, cerebral palsy, and premature birth are also associated with higher squint prevalence. The age at which treatment begins significantly affects outcomes.
In Adults
Adult-onset strabismus can result from thyroid eye disease (Graves’ disease), neurological conditions, diabetes-related nerve damage, head trauma, or stroke. Some adults have a childhood squint that was never fully corrected and becomes more pronounced with age. For adults experiencing double vision, non-surgical options like prism glasses offer immediate symptom relief while the underlying cause is investigated.
Non-Surgical Treatment Options
1. Corrective Glasses
This is the single most effective non-surgical intervention for accommodative squints. When a child’s eyes turn inward because of uncorrected farsightedness, prescribing the right spectacle lenses removes the excessive focusing effort and allows the eyes to straighten naturally. In many cases, glasses alone fully resolve the squint — no therapy, no patching, no surgery. At Visual Aids Centre, a thorough cycloplegic refraction (eye test with dilating drops) is performed to determine the precise prescription.
2. Prism Glasses
Prism lenses bend light before it enters the eye, effectively shifting the image to compensate for misalignment. They don’t cure the squint, but they eliminate double vision and allow the brain to fuse both eyes’ images into a single picture. Prism glasses are particularly useful for small-angle deviations in adults, post-surgical residual misalignment, and as a diagnostic tool to assess whether the brain can achieve binocular fusion. Our customised lens service includes prism prescriptions tailored to individual strabismus profiles.
3. Vision Therapy (Orthoptics)
Vision therapy is a structured programme of eye exercises and activities designed to improve the brain’s ability to control eye alignment and coordination. It’s most effective for convergence insufficiency (difficulty focusing on near objects), intermittent exotropia, and post-surgical fine-tuning. Sessions typically involve pencil pushups (tracking a target toward and away from the nose), stereogram cards, computer-based vergence training, and activities that challenge binocular fusion. At Visual Aids Centre, our vision therapy programme is supervised by trained orthoptists and tailored to each patient’s specific deviation pattern.
4. Patching (Occlusion Therapy)
Patching treats the amblyopia (lazy eye) that often accompanies childhood squints — it doesn’t straighten the eye directly but strengthens the weaker eye’s visual acuity so that binocular vision therapy can work. The stronger eye is covered with an adhesive patch for a prescribed number of hours daily, forcing the brain to engage with the weaker eye. Consistency is critical: skipping patch time delays results. For children concerned about home-based management, patching combined with engaging visual activities (colouring, tablet games with one eye covered) makes compliance easier.
5. Botulinum Toxin (Botox) Injections
Botox can be injected into a specific extraocular muscle to temporarily weaken it, allowing the opposing muscle to pull the eye into better alignment. This isn’t a permanent fix — the effect lasts 3–6 months — but it’s useful for diagnostic purposes (testing whether the eyes can work together if forced into alignment), acute-onset squints (such as those following nerve palsy), and as an alternative to surgery in patients who can’t tolerate general anaesthesia. It’s a clinic-based procedure performed under topical anaesthesia. For patients weighing all options, our detailed guide on squint surgery side effects explains what the surgical alternative involves.
6. Atropine Drops (Penalisation)
As an alternative to patching, atropine drops can be placed in the stronger eye to temporarily blur its vision, encouraging the brain to rely on the weaker eye. This works best in children under 7 with mild-to-moderate amblyopia and is often better tolerated than a patch — there’s nothing to wear or remove, and the child can’t simply peek around it.
When Is Surgery Necessary?
Non-surgical treatments have clear boundaries. Surgery typically becomes necessary when the squint angle is large (greater than 15–20 prism dioptres) and constant, the deviation hasn’t responded to 3–6 months of glasses, therapy, or patching, there’s a structural or anatomical cause that conservative treatment cannot address, or the patient is experiencing persistent double vision that prism glasses cannot adequately correct.
Squint surgery involves tightening or loosening specific extraocular muscles to reposition the eye. It’s performed under general anaesthesia in children and local anaesthesia in adults, with most patients going home the same day. The cost of squint surgery and the expected recovery timeline vary depending on the complexity of the case. For patients considering surgery, understanding the post-operative precautions helps set realistic expectations.
Conclusion
Not every squint requires surgery. Corrective glasses can fully resolve accommodative squints, prism lenses eliminate double vision in small-angle deviations, vision therapy strengthens binocular coordination for intermittent squints, and patching addresses the amblyopia that often accompanies childhood strabismus. The key is an accurate diagnosis — understanding the type, angle, and cause of the squint determines which treatment path makes sense. If you’re unsure whether non-surgical options could work for your case, book a consultation at Visual Aids Centre for a comprehensive strabismus evaluation with our specialist team.
Frequently Asked Questions (FAQs)
Can squint eye be cured without surgery?
Yes, in many cases. Accommodative squints caused by farsightedness often resolve entirely with corrective glasses. Intermittent squints frequently respond to vision therapy and exercises. However, large-angle constant squints usually require surgical correction.
Do eye exercises really work for squint?
They work well for specific types — particularly convergence insufficiency and intermittent exotropia. Pencil pushups, vergence training, and stereogram exercises can measurably improve eye coordination when performed consistently under professional guidance.
At what age should squint treatment begin?
As early as possible. Treatment before age 7 yields the best results because the visual system is still developing. However, adults can also benefit from prism glasses, vision therapy, and Botox injections.
Can a squint come back after non-surgical treatment?
It depends on the cause. If the underlying refractive error changes (e.g., the child’s hyperopia increases), the squint may return until the glasses prescription is updated. Regular follow-ups are essential to monitor stability.
How long does vision therapy take to show results?
Most patients notice improvement within 8–12 weeks of consistent therapy sessions (typically once or twice weekly with daily home exercises). Full results may take 3–6 months depending on the severity of the squint.
👁️ MEDICALLY REVIEWED BY
Padmashree Dr. Vipin Buckshey
Optometrist & Paediatric Vision Specialist | AIIMS Graduate, 1977 | Padma Shri Honouree
With more than four decades of clinical experience and over 250,000 vision correction procedures performed at Visual Aids Centre, Dr. Vipin Buckshey has managed thousands of strabismus cases across all age groups — from infant-onset esotropia to adult-acquired diplopia. An AIIMS alumnus, former President of the Indian Optometric Association, and official optometrist to the President of India, Dr. Buckshey personally oversees the centre’s vision therapy and orthoptics programme, ensuring every squint patient receives a thorough evaluation before any treatment recommendation is made.