If you’ve just had corneal cross-linking (CXL) for keratoconus and your vision is blurry, hazy, or foggy — that’s expected. Cross-linking is designed to stabilise your cornea, not to sharpen your vision overnight. In fact, it temporarily makes vision worse before the cornea settles into its new, stronger state. The question isn’t whether you’ll experience blurred vision after CXL — nearly everyone does — it’s how long it lasts and what the recovery trajectory looks like.
The short answer: most patients regain functional day-to-day vision within two to four weeks, but full visual stabilisation after cross-linking takes three to six months, and in some cases up to a year. The long answer — which this guide provides — depends on whether you had epi-off or epi-on CXL, the severity of your keratoconus before the procedure, and how your individual cornea heals. Below, we break down the specific causes of post-CXL blur, the realistic week-by-week recovery timeline, what you can do to support healing, and the warning signs that something needs attention.
Key Takeaways
- Blurred vision after cross-linking is universal and expected — it peaks in the first week and improves gradually over 1–3 months.
- Epi-off CXL causes more initial blur than epi-on because the epithelium must regenerate (3–5 days), adding a recovery layer.
- Full visual stabilisation typically takes 3–6 months; some patients notice subtle improvements continuing up to 12 months.
- CXL is a stabilisation procedure — the goal is halting keratoconus progression, not necessarily improving visual acuity.
- Persistent worsening of vision beyond one month, significant pain, or new white haze warrants prompt evaluation.
What Is Corneal Cross-Linking and Why Does It Blur Vision?
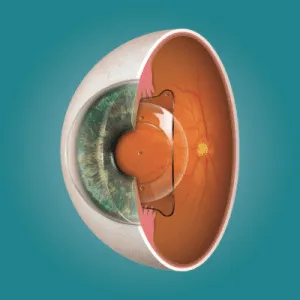
Corneal cross-linking is a procedure that strengthens the collagen fibres within the corneal stroma using a combination of riboflavin (vitamin B2) drops and controlled ultraviolet-A (UVA) light. The UV exposure triggers a photochemical reaction that creates new bonds — “cross-links” — between adjacent collagen strands, making the cornea stiffer and more resistant to further bulging. It’s the primary treatment for halting progressive keratoconus, and it’s also used for post-LASIK ectasia and pellucid marginal degeneration.
The procedure itself is not designed to correct your refractive error — it’s designed to stop your cornea from getting worse. Understanding this distinction is critical to setting realistic expectations. Some patients do experience modest visual improvement after CXL (because the cornea flattens slightly as it stiffens), but many return to approximately the same vision they had before the procedure, just with a stable cornea that no longer deteriorates. The temporary blur you experience during recovery is the healing cost of that stabilisation, and it follows a predictable — if slow — resolution pattern. If you’re exploring whether C3R benefits apply to your situation, this recovery context is essential to understand beforehand.
What Causes Blurred Vision After Cross-Linking?
Epithelial Disruption (Epi-Off)
In the standard epi-off technique, the surgeon removes the corneal epithelium — the outermost protective layer — to allow riboflavin to penetrate the stroma effectively. This leaves the cornea without its smooth optical surface for three to five days while the epithelium regenerates. During this window, vision is significantly blurred and the eye is uncomfortable, similar to a large corneal abrasion. Even after the epithelium closes, it takes weeks for it to smooth out completely and regain uniform thickness.
Corneal Oedema and Stromal Haze
The UV-riboflavin reaction causes controlled damage to the stromal keratocytes (the cells that maintain the cornea’s structural matrix). This triggers an inflammatory healing response — deliberately. The resulting oedema (fluid accumulation) and keratocyte repopulation produce a transient corneal haze that scatters incoming light and degrades visual clarity. This haze is most noticeable in the first one to three months and gradually resolves as new keratocytes mature and the stromal architecture remodels. In some patients, mild haze can persist for six months or longer before fully clearing.
Tear Film Instability
Cross-linking disrupts the corneal nerve plexus, which reduces tear production and blink sensitivity temporarily. An irregular tear film acts as a poor optical surface — light scatters rather than focusing cleanly, producing fluctuating blur that often worsens with prolonged screen use or in dry environments. This component of blur improves as the nerves regenerate over weeks to months.
Temporary Refractive Shift
As the cornea stiffens and remodels after CXL, its curvature changes slightly. This can shift your refraction — sometimes making you temporarily more myopic or increasing astigmatism — before the cornea settles into its final shape. Prescriptions written within the first three months of CXL are therefore unreliable, which is why most surgeons delay new glasses or contact lens fittings until the cornea has stabilised.
Week-by-Week Recovery Timeline
Days 1–5: Peak Blur and Discomfort
This is the hardest phase. If you had epi-off CXL, the exposed cornea is healing its surface layer, and vision is very blurry — reading a phone screen or watching television will be difficult. Pain, light sensitivity, and tearing are normal. A bandage contact lens placed at surgery helps protect the epithelium during regrowth and is typically removed at day three to five once the surface has closed.
Week 1–2: Epithelium Closes, Blur Persists
Once the epithelium has regenerated, the sharp discomfort subsides significantly. Vision remains hazy — better than day one, but far from clear. The corneal stroma is still oedematous, and the newly formed epithelium is irregular. Most patients can navigate their home and manage basic tasks, but driving and detailed work remain difficult. Following the post-CXL precaution guidelines is particularly important during this fragile period.
Weeks 2–4: Gradual Functional Improvement
By the end of the first month, many patients have recovered enough visual clarity for daily activities — reading, screen work, and in some cases driving (depending on baseline vision and local regulations). The cornea is still hazy on slit-lamp examination, but the haze is decreasing. Vision may fluctuate from day to day as the stroma continues remodelling.
Months 1–3: Steady Clearing
This is the period of most noticeable visual improvement. The stromal haze diminishes as new keratocytes repopulate the treated zone, the tear film stabilises, and the refractive shift begins to settle. Patients who wore scleral lenses or rigid contacts before CXL can usually be refitted by the three-month mark, once topography has stabilised enough for accurate lens design.
Months 3–12: Final Stabilisation
For most patients, vision reaches its final post-CXL baseline between three and six months. However, subtle improvements — particularly in corneal haze density and contrast sensitivity — can continue for up to twelve months. The full C3R recovery timeline reflects this extended but diminishing trajectory. If your vision at twelve months is worse than your pre-CXL baseline, your surgeon will investigate whether the procedure has failed to halt progression or whether a comorbid issue needs addressing.
Epi-Off vs Epi-On: How the Technique Affects Recovery
The two main CXL variants have meaningfully different recovery profiles. Epi-off (epithelium-off) CXL is the standard protocol — it removes the epithelium to maximise riboflavin absorption and is the most studied and effective technique for halting keratoconus. The trade-off is a more painful first week and a longer visual recovery, typically two to four weeks to functional clarity and three to six months for full stabilisation.
Epi-on (transepithelial) CXL leaves the epithelium intact, which means less pain and faster initial comfort. However, the epithelium partially blocks riboflavin penetration, which is why modified riboflavin formulations and longer soak times are used. Visual recovery is faster in the first week (there’s no surface defect to heal), but the long-term efficacy data for epi-on is not as robust as epi-off. Your surgeon will choose the technique based on your keratoconus severity, corneal thickness, and specific clinical situation. For an overview of the procedure itself, see our guide on the C3R surgical process.
What You Can Do to Support Healing
You cannot speed up stromal remodelling — that’s a biological process on its own timeline. But you can avoid slowing it down. Use your prescribed steroid drops exactly on schedule; these control the inflammatory response that produces haze, and stopping them early can worsen corneal scarring. Use preservative-free lubricating drops frequently — every one to two hours in the first week, tapering as comfort improves — to maintain a stable tear film and reduce fluctuating blur.
Wear UV-protective sunglasses outdoors for at least the first month; the cornea is photosensitive after riboflavin treatment, and UV exposure during healing can exacerbate haze. Avoid rubbing your eyes — this is critical for keratoconus patients at any time, but especially after CXL when the cornea is actively remodelling. Get adequate sleep, stay well hydrated, and if you’re exploring whether other treatments might complement CXL, read about how C3R compares to other keratoconus management options.
When Blurred Vision After CXL Is Not Normal
Normal post-CXL blur follows a clear pattern: worst in the first week, steadily improving through the first month, and largely resolved by three to six months. If your vision deviates from this trajectory — worsening after the first two weeks rather than improving, or failing to show any meaningful improvement by month two — contact your surgeon. Potential complications include persistent epithelial defects (the surface fails to heal on schedule), sterile corneal infiltrates, infectious keratitis, and excessive stromal haze or scarring.
Severe pain beyond the first three to five days (in epi-off), a visible white spot on the cornea, increasing redness rather than decreasing, or new sensitivity to light that intensifies rather than fades are all reasons for urgent evaluation. Additionally, if topography at three to six months shows continued corneal steepening despite CXL, the procedure may not have been sufficient, and your surgeon will discuss whether additional intervention is needed. Early detection of any complication improves outcomes significantly — don’t skip follow-up appointments.
Conclusion
Blurred vision after corneal cross-linking is a normal, temporary consequence of a procedure designed to save your cornea from progressive keratoconus. The blur results from epithelial disruption, stromal oedema and haze, tear film instability, and temporary refractive shifts — all of which resolve gradually over weeks to months. Most patients regain functional vision within two to four weeks and reach their final visual outcome by three to six months, with subtle improvements possible up to a year. Epi-off CXL has a harder first week but stronger long-term evidence; epi-on is more comfortable initially with a faster early recovery. The key is patience, adherence to your drop regimen, and attending every follow-up. If you’ve been diagnosed with keratoconus and want to understand whether cross-linking is right for your stage, book a consultation at Visual Aids Centre for a personalised assessment.
Frequently Asked Questions (FAQs)
How long does blurred vision last after cross-linking?
Functional vision typically returns within two to four weeks. Full visual stabilisation takes three to six months, with subtle improvements continuing up to twelve months in some patients.
Will my vision improve after cross-linking or just stabilise?
CXL is primarily a stabilisation procedure — it halts keratoconus progression. Some patients experience modest visual improvement as the cornea flattens slightly during stiffening, but the primary goal is preventing further deterioration, not correcting refractive error.
Is epi-off or epi-on cross-linking better for faster recovery?
Epi-on CXL has a faster initial recovery because the epithelium remains intact. However, epi-off CXL has stronger long-term efficacy data. Your surgeon will choose based on your keratoconus severity and corneal thickness.
When can I wear contact lenses after cross-linking?
Most surgeons wait until the cornea has stabilised — typically three months post-CXL — before fitting new contact lenses. Scleral lenses or rigid gas permeable lenses may be recommended for best visual correction.
Is corneal haze after CXL permanent?
In most cases, no. Post-CXL haze peaks at one to three months and gradually resolves as keratocytes repopulate the stroma. Mild residual haze is common but rarely visually significant. Persistent dense haze beyond six months should be evaluated.
Can I drive after cross-linking?
Most patients cannot drive safely in the first one to two weeks. Return to driving depends on your baseline vision and the speed of your recovery — discuss this with your surgeon at your follow-up appointments.
👁️ MEDICALLY REVIEWED BY
Padmashree Dr. Vipin Buckshey
Optometrist & Keratoconus Management Specialist | AIIMS Graduate, 1977 | Padma Shri Honouree
With more than four decades managing progressive corneal conditions and over 250,000 laser vision correction procedures at Visual Aids Centre, Dr. Vipin Buckshey has guided thousands of keratoconus patients through cross-linking and beyond — setting honest recovery expectations based on real-world outcomes rather than textbook averages. An AIIMS alumnus, former President of the Indian Optometric Association, and official optometrist to the President of India, Dr. Buckshey ensures that every CXL patient understands the timeline, the trade-offs, and the follow-up milestones before they enter the procedure room. Learn more about our story.