You are a week out of LASIK surgery, things are going well — and then you notice something in the mirror. One pupil appears slightly larger than the other. Your first thought is panic. Your second thought is whether the surgery caused this. Both reactions are completely understandable, and this guide from Visual Aids Centre is here to give you the clinical reality before anxiety fills in the gaps.
The direct answer: LASIK surgery is highly unlikely to directly cause anisocoria. In the vast majority of cases, what patients notice post-LASIK is either a temporary effect of the anaesthetic drops used during the procedure, a pre-existing condition that was already present, or a variation in pupil size that falls within the normal range of human asymmetry. Genuine, persistent anisocoria caused by the LASIK procedure itself is exceedingly rare — but it is worth understanding exactly why, and what to do if your concern persists.
Key Takeaways
- Anisocoria — unequal pupil sizes — is not a recognised direct complication of LASIK surgery performed correctly by an experienced surgeon.
- Temporary pupil size differences in the first 24–48 hours after LASIK are commonly caused by topical anaesthetic and dilating drops used during the procedure — not by the surgery itself.
- LASIK’s corneal nerve disruption does not directly control pupil size. The pupils are governed by autonomic nerves that the LASIK laser does not reach.
- Pre-existing conditions — Horner’s syndrome, Adie’s pupil, third cranial nerve palsy — may become noticeable for the first time during LASIK recovery, when patients pay close attention to their eyes.
- Any persistent, worsening, or asymmetric pupil change accompanied by headache, pain, or vision deterioration should be assessed by a specialist the same day — not monitored at home.
What Is Anisocoria?
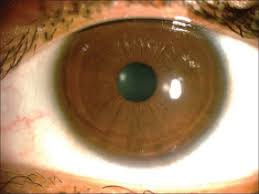
Anisocoria is the medical term for unequal pupil sizes — a condition where one pupil is measurably larger or smaller than the other. It exists on a spectrum. Physiological anisocoria — where the size difference is less than one millimetre and fluctuates naturally — is present in approximately 20% of the general population at any given time and is entirely harmless. Many people have it their whole lives and never notice.
Pathological anisocoria is a different matter. A significant, persistent, or newly developing pupil asymmetry — particularly one accompanied by other symptoms — can indicate underlying conditions ranging from Horner’s syndrome and Adie’s pupil syndrome to third cranial nerve palsy or, in serious cases, intracranial pathology. The clinical context surrounding the pupil asymmetry is what determines whether it warrants immediate specialist attention or reassured monitoring.
What LASIK Does to the Eye — and What It Does Not?
Understanding why LASIK is unlikely to cause genuine anisocoria requires a basic understanding of what the procedure actually changes. LASIK reshapes the cornea — the clear dome at the front of the eye — by applying laser energy to the stromal tissue beneath a thin hinged flap. The cornea’s job is to refract light correctly onto the retina. The procedure improves vision by changing the geometry of that refraction.
Pupil size is not governed by the cornea. It is controlled by the autonomic nervous system through two muscle systems in the iris: the dilator pupillae (which enlarges the pupil) and the sphincter pupillae (which constricts it). These muscles are regulated by the sympathetic and parasympathetic branches of the autonomic nervous system via pathways that do not pass through the corneal stroma. The LASIK laser operates within the cornea’s anterior tissue — it does not reach, interact with, or damage the autonomic neural pathways that control pupil diameter.
The Link Between LASIK and Anisocoria — What Actually Causes Post-Op Pupil Changes?
Temporary Pupil Reaction From Procedure Drops
During LASIK, topical anaesthetic drops and dilating drops are applied to the eye. Dilating agents — typically tropicamide or phenylephrine — temporarily enlarge the pupil to facilitate examination and procedure set-up. In the hours following surgery, as these drops metabolise, the pupil in the treated eye may return to its normal size at a slightly different rate than the untreated side, or compared to how it behaves on subsequent days. This asymmetry is pharmacological, not neurological — it resolves within hours to a day and does not represent anisocoria in any clinically meaningful sense.
Corneal Nerve Disruption — an Indirect Effect
LASIK does disrupt corneal nerves — the sensory nerves responsible for tear film signalling and blink reflex. This nerve disruption is the mechanism behind the post-operative dry eye that most LASIK patients experience to some degree in the first weeks and months. It is worth noting, however, that these are sensory corneal nerves — not the autonomic nerves that control pupil size. The nerve disruption does not directly affect pupillomotor function. What it can do, in rare circumstances, is cause ocular surface discomfort that influences how light appears to the patient — which is sometimes subjectively interpreted as a visual asymmetry, not a genuine pupil size difference.
The broader context of how LASIK affects corneal nerves and the downstream effects of that disruption — including the dry eye timeline — is one of the most important things patients can understand before surgery. Our resource on LASIK surgery complications gives a complete clinical picture of which complications are documented, how frequently they occur, and how they are managed when they do.
Pre-Existing Conditions Unmasked
This is one of the more nuanced aspects of the LASIK-anisocoria connection, and it is clinically important. Conditions such as Horner’s syndrome, Adie’s pupil syndrome, or physiological anisocoria may have been present in a patient for years — even a lifetime — without their knowledge. LASIK creates a period of intense ocular self-scrutiny. Patients examine their eyes closely in the mirror multiple times a day during recovery, looking for changes. This heightened observation frequently reveals pre-existing asymmetries that were always there but never noticed in ordinary daily life. The LASIK did not cause these conditions — the recovery experience simply provided the first occasion on which the patient looked carefully enough to detect them.
How Rare Is LASIK-Related Anisocoria?
Genuine, persistent anisocoria directly caused by LASIK — as opposed to the transient pharmacological effect of procedure drops or the discovery of pre-existing asymmetry — is not a recognised complication in large LASIK outcome studies. The procedure’s reported overall complication rate is low, and pupil irregularities from the surgery itself are not a documented category in FDA reports or major multicentre outcome datasets.
LASIK’s overall patient satisfaction rate exceeds 95% in published clinical studies — a figure that reflects not just vision outcomes but the complete patient experience including recovery. Our guide on night vision after LASIK addresses the visual quality concerns that patients most commonly report in the first weeks post-operatively — including halos, glare, and the light-sensitivity that is sometimes confused with pupil abnormality.
Other Causes of Unequal Pupils Post-LASIK
If pupil asymmetry appears or becomes noticeable during LASIK recovery, the surgery should not be assumed to be the cause before these alternatives are considered:
- Medications: Antihistamines, glaucoma drops, and several systemic medications can alter pupil reactivity or size — creating apparent asymmetry that has nothing to do with LASIK. A full medication review is always relevant when anisocoria is newly noted.
- Neurological conditions unrelated to surgery: Third cranial nerve palsy and Horner’s syndrome can develop or become apparent at any time. Their timing coinciding with LASIK recovery does not make LASIK the cause.
- Physical trauma during recovery: An accidental bump to the eye area — walking into a door frame, rubbing too firmly — can cause transient iris or ciliary muscle dysfunction that affects pupil reactivity temporarily.
- Psychological stress: Acute stress and heightened anxiety can stimulate sympathetic nervous system activity, producing mild bilateral pupil dilation that may appear asymmetric in certain lighting conditions.
Understanding the full risk landscape before LASIK — including which pre-existing conditions could become apparent during recovery — is part of what a thorough pre-operative assessment addresses. Our resource on LASIK eye surgery risks explains the complete risk profile with honest clinical context.
Symptoms That Warrant Same-Day Medical Attention
Most post-LASIK pupil observations are benign and resolve without intervention. The following symptoms are different — they indicate that the asymmetry may reflect something clinically significant that requires prompt evaluation:
- Unequal pupils that do not resolve within 48 hours of surgery and cannot be explained by procedure drops wearing off
- A drooping eyelid (ptosis) on the same side as the larger or smaller pupil — this combination is a hallmark of Horner’s syndrome
- Double vision or significant loss of visual clarity in addition to pupil asymmetry
- Severe headache — particularly a sudden, severe headache unlike anything experienced before — which can indicate an intracranial pressure event
- Significant eye pain beyond the expected grittiness of normal post-operative recovery
Any of these in combination with pupil asymmetry is a same-day medical emergency. Do not monitor overnight and reassess — contact your ophthalmologist or go directly to an emergency eye unit.
What to Do If You Suspect Anisocoria After LASIK?
If you notice what appears to be unequal pupil sizes after LASIK, follow this practical response sequence:
- Photograph both eyes in neutral, consistent lighting — this gives you a baseline record and helps your ophthalmologist assess whether any subsequent change has occurred.
- Note timing — when did you first notice it? Has it changed? Is it the same in both bright and dim lighting? Pupil asymmetry that is equal in both bright and dark conditions has different diagnostic implications from asymmetry that changes with lighting.
- Review your medications — check whether anything you have taken recently could affect pupil size.
- Contact your Visual Aids Centre team at the first review appointment — or sooner if any of the serious symptoms described above are present.
- Do not self-diagnose from general internet searches. Anisocoria has a very wide differential — from completely benign to serious neurological emergency. Only a clinical examination can distinguish between them.
Preventative Measures for Safer LASIK Outcomes
While LASIK-related anisocoria is not a standard complication risk, the broader principle of preventing post-operative concerns applies fully here. The steps that give you the best possible LASIK outcome are also the steps that minimise the chance of any post-operative concern becoming a complication:
- Complete and honest medical history disclosure at your pre-operative assessment — including any prior neurological symptoms, history of eye trauma, medications, and family history of eye conditions
- Choose an experienced, qualified surgeon operating in an environment with comprehensive pre-operative assessment tools. Our guide on how to choose the right LASIK surgeon covers what experience markers and facility standards to evaluate
- Follow all post-operative care instructions precisely — including the drops schedule and activity restrictions
- Attend every follow-up appointment — monitoring is where early concerns are caught and managed before they become clinical problems
Conclusion
LASIK surgery does not directly cause anisocoria in the clinical sense. The procedure does not reach or interact with the autonomic neural pathways that govern pupil size. Temporary pupil asymmetry in the immediate post-operative period is typically pharmacological — a transient effect of the procedure drops that resolves within hours. Persistent pupil asymmetry following LASIK is more likely to reflect a pre-existing condition newly noticed during the heightened self-observation of recovery than a complication of the surgery itself.
If you are concerned about pupil changes after LASIK, the right response is to document them, report them to your ophthalmologist, and allow a clinical examination to distinguish reassurance from action. Book an appointment at Visual Aids Centre for any post-operative concern — our team would rather see you and reassure you than have a question go unexamined.
Frequently Asked Questions (FAQs)
Can LASIK directly cause anisocoria?
LASIK is highly unlikely to directly cause anisocoria. The laser operates within the corneal stroma and does not interact with the autonomic nerves that control pupil size. Temporary pupil asymmetry immediately after surgery is almost always caused by the dilating drops used during the procedure.
Why do my pupils look unequal after LASIK?
The most likely explanation in the first 24–48 hours is residual asymmetric effect from the topical dilating drops applied during surgery. These wear off at slightly different rates between eyes. If the asymmetry persists beyond 48 hours, contact your ophthalmologist for assessment.
Is anisocoria after LASIK dangerous?
Temporary, pharmacologically-caused pupil asymmetry is not dangerous. Persistent anisocoria accompanied by headache, ptosis (drooping eyelid), double vision, or pain warrants same-day emergency evaluation as these symptom combinations can indicate neurological conditions unrelated to LASIK that require urgent management.
What should I do if I notice unequal pupils after LASIK?
Photograph both eyes, note when you first observed the asymmetry, and contact your ophthalmologist. Do not wait for a scheduled appointment if you have accompanying symptoms like headache, pain, or vision changes. A clinical examination is the only reliable way to determine the cause.
Can pre-existing conditions cause anisocoria to appear after LASIK?
Yes — this is one of the more common explanations. Conditions like physiological anisocoria, Horner’s syndrome, or Adie’s pupil may have been present for years without the patient noticing. The heightened self-observation during LASIK recovery frequently brings these pre-existing asymmetries to attention for the first time.
Does LASIK’s corneal nerve disruption affect pupil size?
No. LASIK disrupts sensory corneal nerves — those responsible for tear film signalling and the blink reflex. These are not the same neural pathways that control pupil dilation and constriction, which are governed by autonomic sympathetic and parasympathetic fibres that the LASIK laser does not reach.
👁️ MEDICALLY REVIEWED BY
Padmashree Dr. Vipin Buckshey
BS Ophthalmology | AIIMS Graduate, 1977 | Padma Shri Honouree | Post-LASIK Neurological Symptom Assessment Specialist, Visual Aids Centre
Patients who notice unusual symptoms during LASIK recovery — especially symptoms involving the pupil or visual system — frequently encounter information online that generates more anxiety than clarity. Dr. Vipin Buckshey’s clinical approach at Visual Aids Centre is grounded in a different principle: patients who understand exactly what LASIK does and does not do to the eye’s neural architecture can self-assess symptom significance far more accurately than those who rely on generalised medical information designed for a different patient population. His background in both refractive surgery and the broader neuro-ophthalmic complications framework — built over four decades of post-operative review and complex case management — is the evidence base for the clinical guidance in this article. An AIIMS alumnus, Padma Shri honouree, and former President of the Indian Optometric Association. Learn more about our post-operative care approach at our story.