You had LASIK years ago and it worked well — until it didn’t. Maybe your prescription has drifted back, or you’re dealing with residual myopia that a touch-up can’t safely fix because there isn’t enough corneal tissue left. The question now is whether an Implantable Collamer Lens can pick up where LASIK left off.
The short answer is yes — ICL surgery after LASIK is not only possible, it is a well-established clinical pathway for patients who need further vision correction but are no longer candidates for additional corneal laser treatment. The lens sits behind the iris and in front of your natural lens, correcting the refractive error without removing any more corneal tissue. This guide explains who qualifies, what your surgeon needs to evaluate, how the procedure works differently after prior LASIK, and what results you can realistically expect. If you are weighing your options, our detailed ICL versus LASIK comparison covers the broader differences between these two procedures.
Key Takeaways
- ICL can be safely implanted after LASIK — the two procedures affect different parts of the eye and do not interfere with each other.
- The most common reason for ICL after LASIK is residual or recurrent myopia that cannot be corrected with a laser enhancement due to insufficient corneal thickness.
- Your surgeon must confirm corneal stability, adequate anterior chamber depth, healthy endothelial cell count, and a stable prescription before proceeding.
- ICL after LASIK achieves excellent visual outcomes — most patients reach 6/6 (20/20) or better — and the lens is fully reversible if needed.
Why Would You Need ICL After LASIK?
LASIK permanently reshapes the cornea, but the eye itself continues to change over time. Several scenarios can leave a previous LASIK patient with vision that is no longer sharp enough to go without glasses.
Myopic Regression
A small percentage of LASIK patients experience a gradual return of nearsightedness as the cornea subtly steepens over the years. If the regression is mild (under –1.00 D), a laser enhancement can usually correct it. But if it exceeds what the remaining corneal tissue can safely support, a corneal-based retreatment is off the table.
Insufficient Corneal Thickness for Enhancement
Every LASIK procedure removes a measured amount of stromal tissue. A second ablation requires enough residual tissue to remain structurally safe — typically a minimum of 250 microns beneath the flap. If your corneal thickness measurements show there isn’t enough tissue for a safe retreatment, ICL bypasses the cornea entirely.
High Residual Prescription
Sometimes the original LASIK under-corrected a very high prescription, or the patient’s myopia has progressed significantly since surgery. For patients whose remaining error is –3.00 D or more, ICL is often a better solution than pushing the limits of corneal ablation. Our article on what happens when prescriptions exceed LASIK’s range explains where the boundaries of laser correction lie.
Presbyopia and Age-Related Changes
Patients who had LASIK in their twenties or thirties may find that by their mid-forties, the combination of a mild prescription shift and emerging presbyopia makes distance or near vision frustrating. ICL — or in some cases refractive lens exchange — can address this, especially when the cornea is no longer an ideal treatment surface.
How ICL Works Differently from LASIK
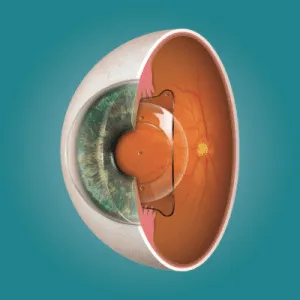
This distinction is crucial: LASIK reshapes the cornea’s surface to redirect light. ICL does not touch the cornea at all. Instead, a thin, flexible lens made of Collamer (a biocompatible collagen copolymer) is placed inside the eye through a micro-incision of approximately 2.8 mm. The lens sits in the posterior chamber — the space between the iris and your natural crystalline lens.
Because the cornea remains untouched, ICL avoids the structural concerns that make a second LASIK risky. There is no additional thinning, no flap-related complications, and no worsening of any post-LASIK dryness. In fact, ICL is often better tolerated than laser enhancement precisely because it does not further compromise corneal nerves. For patients who have already dealt with post-LASIK dry eye, this is a meaningful advantage.
The other important difference is reversibility. A corneal laser procedure permanently removes tissue — there is no putting it back. An ICL can be removed or exchanged if your prescription changes significantly or if you eventually need cataract surgery. This flexibility is one of the reasons surgeons increasingly recommend ICL for post-LASIK patients rather than pushing the boundaries of what the cornea can safely tolerate. For a side-by-side breakdown, our EVO ICL versus LASIK comparison covers both procedures in detail.
What Your Surgeon Evaluates Before ICL After LASIK
Not everyone who has had LASIK automatically qualifies for ICL. The pre-operative evaluation is thorough — and in some respects more detailed than a first-time ICL assessment, because your surgeon needs to account for the corneal changes from the previous procedure.
Corneal Stability and Topography
The cornea must be stable — no progressive thinning or ectasia. A Pentacam scan maps the full thickness and curvature of the cornea, checking for any irregularities that developed after LASIK. If there are signs of post-LASIK ectasia, that must be addressed (potentially with corneal cross-linking) before an ICL can be safely implanted.
Anterior Chamber Depth
The ICL needs physical space inside the eye to sit safely without touching the natural lens or the back of the cornea. A minimum anterior chamber depth of 2.8 mm (measured from endothelium to lens) is typically required. This measurement is unaffected by prior LASIK in most cases.
Endothelial Cell Count
The endothelial cells lining the inner cornea are responsible for keeping the cornea clear. If the count is too low (usually below 2,000 cells/mm²), an ICL placed in close proximity could risk further cell loss over time. Your surgeon will perform specular microscopy to verify this.
Prescription Stability
Your refractive error must be stable for at least twelve months. If your prescription is still drifting — whether from ongoing regression or a separate cause — implanting a lens to a moving target will produce unsatisfying results. Patients who are uncertain whether their vision has settled can read our article on whether eyes can deteriorate again after LASIK for a clearer picture of long-term stability.
Cataract Status
ICL is placed in front of the natural lens, so early cataract development can complicate the picture. If there are signs of lens opacity, your surgeon may recommend cataract surgery with a premium IOL instead — solving both the cataract and the refractive error in one procedure.
What the ICL Procedure Looks Like After Previous LASIK
The surgical technique is essentially the same as a primary ICL implantation. The procedure takes approximately 15–20 minutes per eye and is performed under topical anaesthesia (numbing drops — no injections). A micro-incision is made at the corneal periphery, the folded ICL is inserted through it, and the lens unfolds and is positioned behind the iris. No sutures are needed — the incision self-seals.
The one consideration unique to post-LASIK patients is the existing corneal flap. Your surgeon will place the incision away from the flap edge and handle the eye gently to avoid any inadvertent flap disturbance, though the risk is extremely low since most LASIK flaps are well-healed by the time ICL is considered (typically years later).
Recovery is rapid. Most patients notice dramatically improved vision within hours. A short course of antibiotic and anti-inflammatory drops is prescribed, and follow-up visits are scheduled at day one, one week, one month, and then periodically thereafter. If you are already familiar with post-LASIK recovery, you will find ICL recovery faster and more comfortable — there is no flap healing, no surface ablation discomfort, and dry eye symptoms are typically minimal.
What Results Can You Expect?
The published outcomes for ICL after LASIK are excellent. Studies consistently report that over 90% of patients achieve uncorrected visual acuity of 6/6 (20/20) or better, with high levels of patient satisfaction. The predictability of ICL is particularly strong because the lens power can be calculated precisely — unlike a laser enhancement, where the corneal healing response after a previous ablation can introduce variability.
Patients also report improved contrast sensitivity and visual quality compared to wearing glasses or contacts over a post-LASIK cornea. The ICL creates a smooth optical correction inside the eye, bypassing any subtle corneal irregularities left from the original procedure. For patients who experienced mild ghosting or image doubling after LASIK, ICL can sometimes improve these symptoms as well.
Long-term data (ten years and beyond) confirms that ICLs remain stable, with minimal vault change and no significant endothelial cell loss when proper sizing protocols are followed. The lens does not degrade, does not require maintenance, and does not develop deposits or coatings.
When ICL Isn’t the Right Choice — and What Is
ICL is not always the answer. If your residual prescription is small (under –1.50 D) and your cornea has adequate thickness, a LASIK enhancement or surface ablation may be simpler and equally effective. If you are over 50 with early lens changes, a refractive lens exchange might address both the prescription and emerging cataracts in one step.
For patients with irregular astigmatism from the original LASIK that cannot be corrected by a spherical or toric ICL, specialty contact lenses like sclerals may provide better visual quality than any surgical option. Your surgeon at Visual Aids Centre will map out every viable pathway and recommend the one that gives the sharpest, safest outcome for your specific situation.
Conclusion
Yes, you can have ICL after LASIK — and for many patients, it is the safest and most effective way to regain clear vision when a laser enhancement is not feasible. The two procedures work on completely different parts of the eye: LASIK reshapes the cornea, ICL sits inside the eye behind the iris. Because no additional corneal tissue is removed, ICL preserves the structural integrity of a cornea that has already been treated. The key requirements are a stable prescription, adequate anterior chamber depth, healthy endothelial cells, and a thorough evaluation by a surgeon experienced in both refractive platforms. If your vision has changed since LASIK and you want to explore whether ICL is right for you, get in touch with Visual Aids Centre for a comprehensive assessment.
Frequently Asked Questions (FAQs)
Is ICL surgery safe after LASIK?
Yes. ICL does not touch the cornea, so it does not interact with the previous LASIK flap or ablation zone. Published safety data for ICL after LASIK is comparable to primary ICL implantation.
How long after LASIK can I get ICL?
There is no strict minimum, but most surgeons recommend waiting at least 12 months to ensure your prescription has fully stabilised after LASIK. In practice, most patients seeking ICL are years or decades post-LASIK.
Will the LASIK flap be affected during ICL surgery?
No. The micro-incision for ICL is made at the corneal periphery, well away from the central flap zone. The flap is typically fully healed by the time ICL is considered.
Can ICL correct astigmatism left over from LASIK?
Yes. Toric ICL models are available and can correct residual astigmatism of up to 4–5 dioptres alongside myopia or hyperopia.
Is ICL after LASIK reversible?
Yes. Unlike corneal laser procedures, ICL can be removed or exchanged at any time if your vision needs change or if you require cataract surgery in the future.
What if my cornea is too thin for both LASIK enhancement and ICL?
Corneal thickness does not affect ICL eligibility — the lens bypasses the cornea entirely. If your anterior chamber depth and endothelial cell count are adequate, thin corneas are actually one of the strongest indications for choosing ICL.
👁️ MEDICALLY REVIEWED BY
Padmashree Dr. Vipin Buckshey
Optometrist & Refractive Surgery Specialist | AIIMS Graduate, 1977 | Padma Shri Honouree
With more than four decades of clinical experience and over 250,000 laser vision correction procedures performed at Visual Aids Centre, Dr. Vipin Buckshey and the surgical team have managed thousands of patients requiring secondary refractive procedures — including ICL implantation after prior LASIK. An AIIMS alumnus, former President of the Indian Optometric Association, and official optometrist to the President of India, Dr. Buckshey personally evaluates every post-LASIK ICL candidate to ensure the safest and most effective pathway back to clear vision. Learn more about our team and clinical philosophy.